On the welcome page of the dictionary, four major sections are shown: Normal tissues, Cancer, Cell structure and Protein expression. Below the image of each section are links to introductory texts for i) normal tissue histology, ii) hallmarks of cancer, and iii) cell structure overview. For the cancer-section there is also a link to current cancer statistics (incidence, survival, etc) for Sweden and the rest of the world. Below the Protein expression section there is a list of genes with links to examples of different protein expression patterns. Within each section there are direct links to histology descriptions of different tissue types and tumor forms as well as descriptions of cell structures.
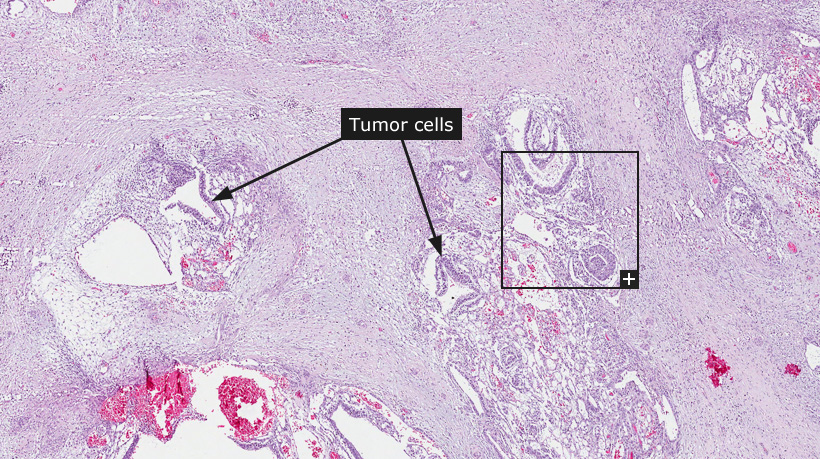
For the 'Tissue & cell types' and 'Tumors' sections, tissue-slides stained with hematoxylin and eosin (HE) are shown at three different levels of magnification. On the top level, an overview of the whole tissue-sample is shown with boxes in black indicating where zoomed-in representative parts of the tissue are available for viewing. Clicking on these boxes will zoom in on that part to show tissue structures, cells and features in greater detail. Throughout these sections, arrows indicate relevant tissue structures, cell-types and other features.
For the 'Cell structure' section, immunofluorescent images of formaldehyde-fixed cell lines are shown. The various cell structures that are demonstrated are always shown in the green channel using an antibody found in the Human Protein Atlas. The antibody name is linked to the subcellular location summary page of the target gene. The other channels: nucleus, microtubules and endoplasmic reticulum, are always shown in the blue, red and yellow channels, respectively. The channels can be toggled on and off by clicking on the respective coloured button above the image. When applicable, the immunofluorescent images are complemented by immunohistochemically stained cells where the location of the particular cell structure is shown in brown.
For the 'Protein expression' section, tissue slides representing both normal and cancer tissue have been stained using immunohistochemistry to visualize various protein expression patterns. Antibodies have been selected to demonstrate the expression patterns of well-known proteins and to reflect antibodies used in clinical diagnostics to determine the nature of a given cancer. For certain antibodies the corresponding protein expression pattern is shown in both normal and cancer tissues. For each exemplified protein there is a short descriptive text including also the clinical usefulness of the corresponding antibody.
A common feature for all sections is that a general descriptive text about the tissue, tumor-type, cell structure or protein/antibody is provided when browsing a particular topic.